
Bumetanide, A Diuretic, Reduces Core Symptoms Of Autism: The French Connection
by James O’Hanlon, Ph.D., Psychopharmacologist
French medical scientists seem to have a knack for appreciating the properties of drugs, developed for other purposes, which make them suitable for treating neuropsychiatric disorders. The classic example was their recognition in 1952 that chlorpromazine, initially developed as an antihistamine, was uniquely effective for treating schizophrenia. The French may have done it again, this time for autism.
Eric Lemonnier, a child psychiatrist, is the central figure in this story. During the time he worked at the French equivalent of a Regional Center, Lemonnier attended a presentation by neurologist Yezkhel Ben-Ari. It concerned the generally unrecognized potential of bumetanide for treating many brain disorders. Lemonnier grasped the implications for the treatment of autism and elicited Ben-Ari’s collaboration. After preliminary studies, they undertook a series of clinical trials that have grown in size and sophistication over the past decade. The most recent shall be described shortly but first, what is bumetanide?
Bumetanide has been used since 1975 as a diuretic for reducing edema due to heart, kidney or liver failure. The drug acts by inhibiting a family of distinct proteins, called cotransporters, which span the plasma membranes of cells to allow the influx of specific ions. At a rate of 1-3 times per second, these cotransporters carry one sodium (Na+), one potassium (K+) and two chloride ions (Cl– ) into cells. There are two members of the family named for the ions transported and distinguished by their order of discovery; i.e., NKCC1 and NKCC2. NKCC1 is expressed in numerous organs, including the brain, whereas NKCC2 is expressed exclusively by nephrons in the kidney. Nephrons are the urine-forming units of the kidney. Each nephron filters water, ions and other solutes from the blood, directing the stream through a conduit lined with specialized cells that extract solutes, returning them to the blood. Water follows the solutes by osmosis as the stream condenses into urine. Multiple transporters, including NKCC2, are involved in the extraction process. By inhibiting NKCC2, bumetanide increases the urine volume up to 20%, albeit with some detrimental ion wastage, particularly that of K+. The drug’s diuretic effect is irrelevant to any therapeutic effects it may have in autism but is important for understanding its side effects.
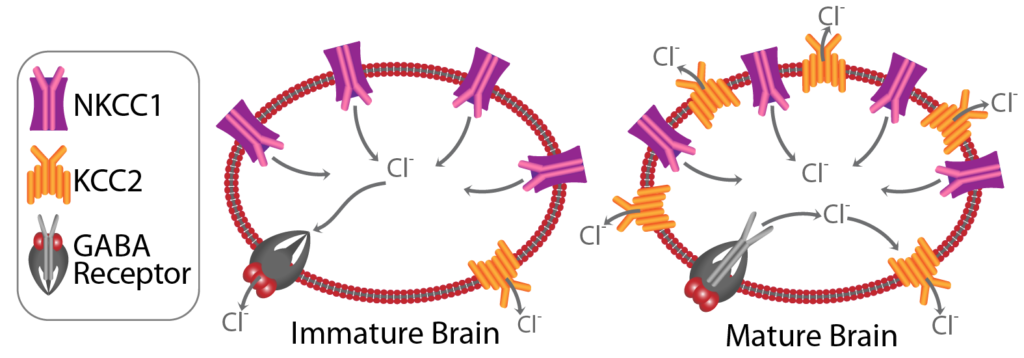
The figure illustrates the function of NKCC1 in two stages of brain development. In both stages NKCC1 transports Cl– into neurons. Its effect on the neuronal chloride concentration is balanced by that of another cotransporter, KCC2. Whereas NKCC1 controls Cl– influx, KCC2 controls Cl– efflux. Together, the cotransporters regulate the internal neuronal Cl– concentration. However, the balance between neuronal influx and efflux changes with brain maturation. Finalization of connections between neurons occurs during late fetal development and for several postnatal weeks. During this immature stage, neurons express NKCC1 abundantly but express KCC2 to a much lower extent. Consequently the internal neuronal Cl– concentration is higher than that in the external milieu. This affects the neuron’s response to the neurotransmitter, γ-aminobutyric acid (GABA). GABA acts upon a particular receptor to open a chloride channel through the neuronal membrane allowing Cl– to flow out of the neuron. The effect is excitatory making it more likely that the neuron conduct a signal to other neurons. As the brain matures, KCC2 is also expressed abundantly and internal neuronal Cl– concentration falls below that in the external milieu. GABA still opens the channel but the direction of the Cl– flow is reversed. Now the effect is inhibitory and will remain so for duration of life. At least that is what normally happens. The French suspected that this developmental switch is poorly executed in the autistic brain. Consequently, a pathological situation exists whereby GABA remains excitatory in some proportion of the neuronal population. They sought to compensate for the supposed predominance of NKCC1 over KCC2 by blocking the former with bumetanide.
The latest French study1 was a multicenter double-blind, placebo-controlled, trial. The purpose was to evaluate the efficacy and safety of three doses of bumetanide to select the optimum dose for use in subsequent trials. Participants were 88 children and adolescents with severe autism aged 2-17 years. They were randomly assigned to four groups who received placebo or bumetanide in doses of 0.5, 1.0 or 2.0 mg, twice daily, for 90 days. Standard scales were used for measuring changes in autistic symptoms from baseline to the final day of treatment. The Childhood Autism Rating Scale (CARS), measuring stereotyped behavior, deficient communication and impaired social interaction, was deemed the most important. Improvement on CARS and two supporting scales was significantly greater after bumetanide than placebo. All bumetanide doses produced similar degrees of improvement. For participants who completed the trial, 62% of those receiving bumetanide verses 19% of those given placebo qualified as “responders” by exceeding a pre-established criterion for improvement on CARS. Psychiatrists rating overall change in participants’ behavior on a 7-level scale found that 33% of the bumetanide-completers but only 5% of the placebo-completers were “much” or “very much” improved. But fewer participants completed the trial while taking bumetanide in medium (83%) and highest (59%) doses than those taking the lowest dose (100%) or placebo (91%). Side effects related to the drug’s diuretic activity were the main reason for attrition at higher doses. So, bumetanide reduces the core symptoms of autism but only in children and adolescents who can tolerate it.
Identification of NKCC1 as the target for drugs that reduce core symptoms of autism is a major achievement of French research. Also important is the indication of dysregulated neuronal Cl– transport in autism. Least important is the drug Lemonnier and Ben-Ari employed for validating their concept. They chose bumetanide because it is the most selective NKCC1 inhibitor currently available. Yet it also inhibits NKCC2; fine for diuretic purposes but definitely unwanted for treating autism. It would be surprising if pharmaceutical companies were not already engaged in developing drugs that specifically inhibit NKCC1. The first to gain official approval for the treatment of autism would be the real breakthrough. In the meantime, there is bumetanide.
1 Lemonnier E, Villeneuve N, Sonie S, et al. Effects of bumetanide on neurobehavioral function in children and adolescents with autism spectrum disorders. Translational Psychiatry (2017) 7, e1056; doi: 10.1038/tp2017.10